The thing about HCCT 2026 that stuck with me wasn't a single session. It was a sentence I heard, in some form, at nearly every table: agentic AI for patient access is not the future. It is here now, and health systems are already using it to take pressure off teams they cannot staff fast enough.
That shift in tone is the story. A year ago the question in these rooms was whether AI agents belonged in patient access at all. This year the room had moved on. The energy was high and the sessions were full, and the people in them were comparing notes on how they are already running it.
Who was there
I spent most of the conference talking with patient access leaders from different health systems. The titles ranged from Director of Contact Center to Director of Patient Access Quality and Training to VP of Patient Access Contact Centers. Different sizes, different EHR setups, but the same core problem on everyone's mind: call volume keeps climbing, schedulers are hard to hire and harder to keep, and adding headcount has stopped being a realistic answer.
What the sessions kept circling back to
Two themes ran through almost every conversation:
- Epic integration. Leaders did not want a bolt-on that lives next to their EHR. They wanted AI agents that work inside the Epic workflows their teams already use, so the automation shows up where the work actually happens.
- Using AI to reduce burnout. This came up as often as cost did, and sometimes ahead of it. The framing was less "cut the queue" and more "give my staff their day back." When routine calls get handled automatically, the people who stay get to spend their time on the complex, patient-specific work that drew them to the job in the first place.
The session people were talking about afterward: Nebraska Medicine
Pat Michael and Matt Kurtz from Nebraska Medicine walked the room through how they built AI agents into their two contact centers on Epic, then did the thing most conference talks don't: they put the numbers on the screen.
They opened with the challenge, and it landed because every patient access leader in the room already lives it. It is difficult and getting harder to find and retain staff. Call volumes keep rising, which pushes up wait times, call abandonment, and access problems, which in turn burns out the staff who remain and chips away at the patient experience.
Then they showed where they landed after building the agents in:
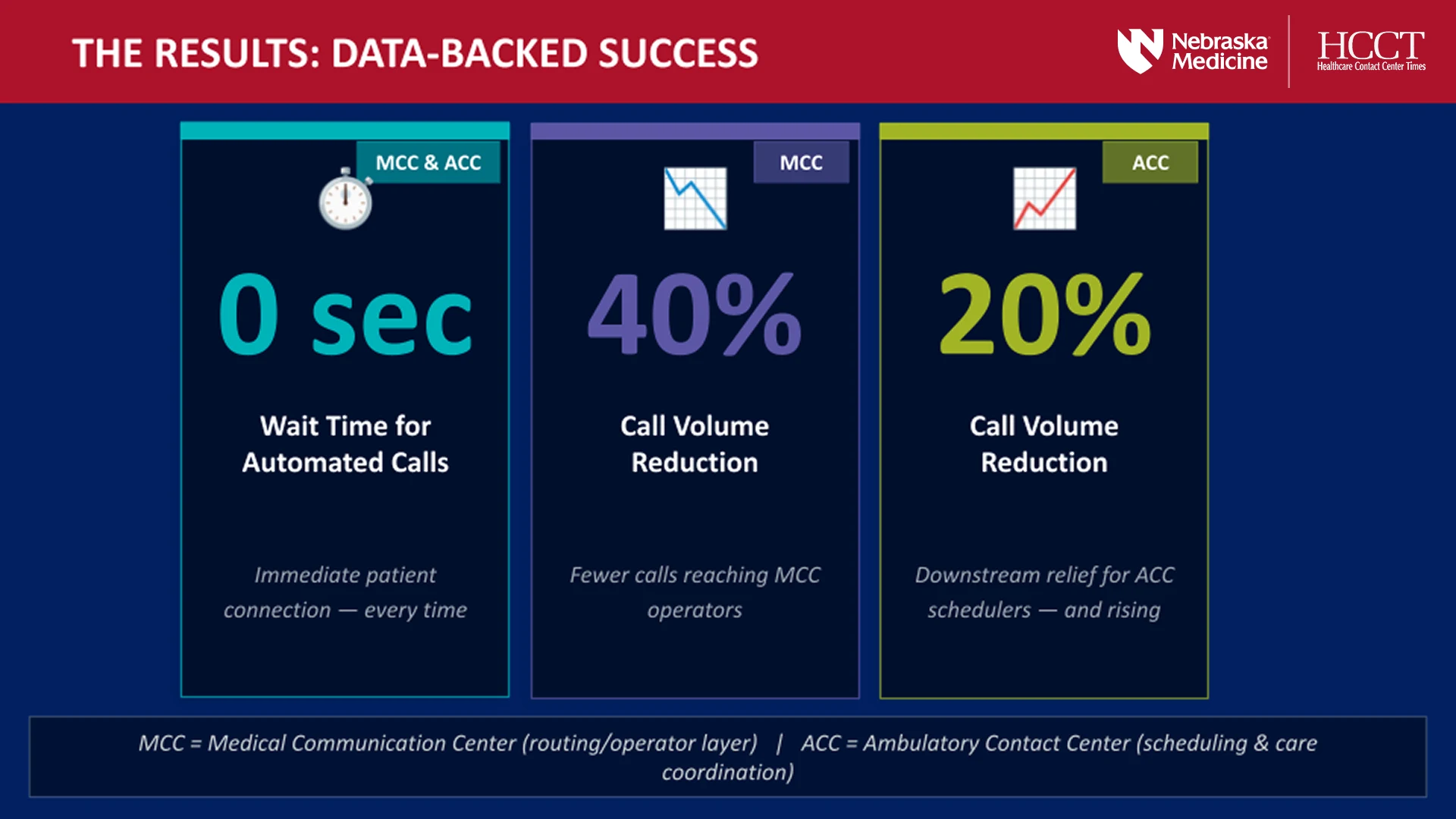
- 0 seconds of wait time on automated calls. Every time.
- 40% fewer calls reaching the hospital operator line, their Medical Communication Center.
- 20% fewer calls into the ambulatory scheduling center, and still dropping.
What made the talk land wasn't the technology. It was what the agents handed back to the staff.
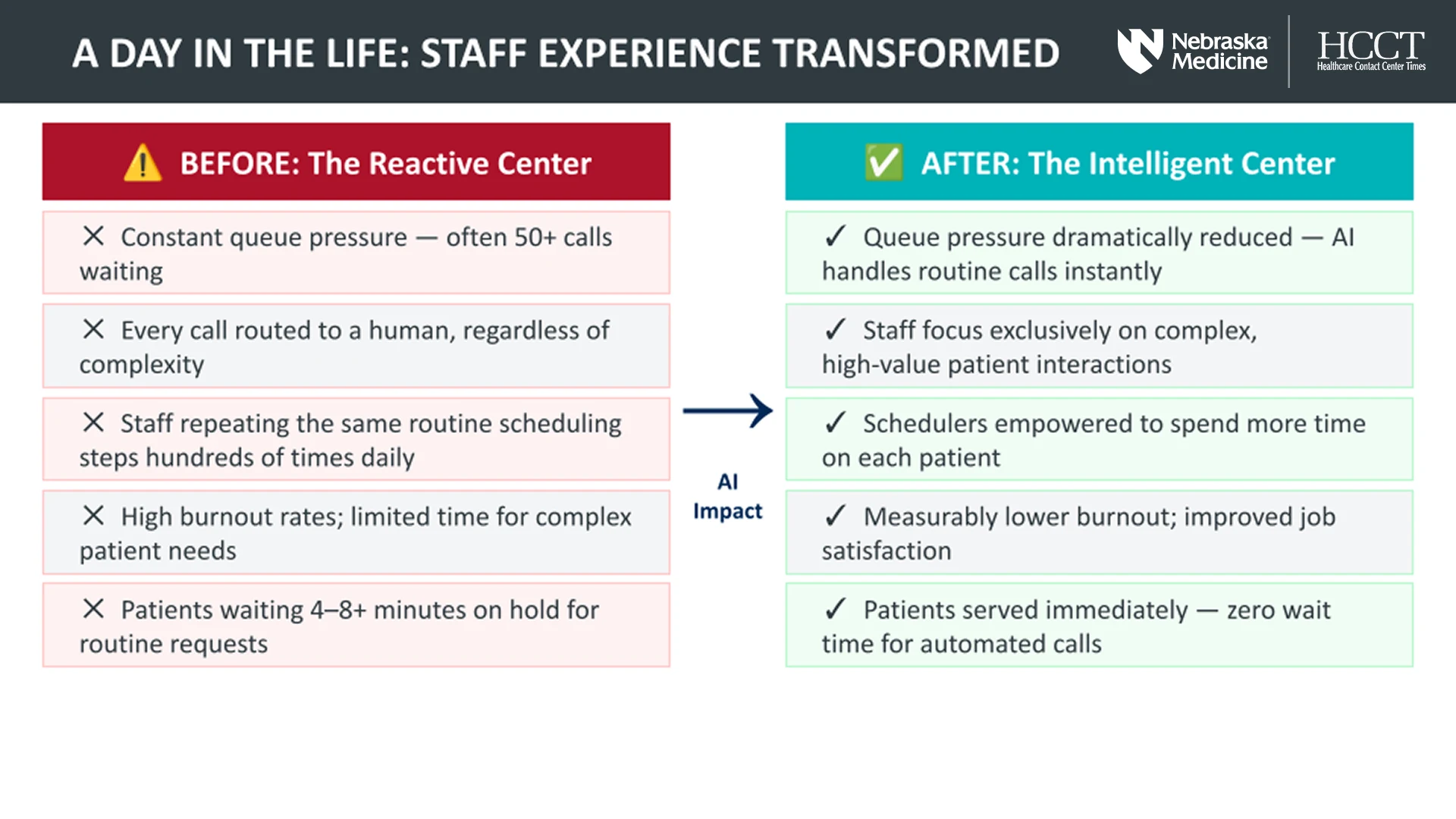
Before, schedulers spent the day repeating the same routine steps over and over against a queue that never emptied. After, the routine calls get answered instantly, and schedulers spend their time on the complex, high-value interactions that actually need a person. The patient experience improved on both ends: faster answers for the simple requests, and a real person with time to help on the hard ones.
"Agentic AI for patient access is not vaporware. It is delivering real value today, helping health systems reduce staff burnout while creating a differentiated patient experience. Every system in that room is staring at the same wait-time math, and Nebraska Medicine showed you can take real volume off your busiest queues without the experience ever feeling automated." Daniel McDuffie, Vice President, Sales at ActiumHealth
The framing Pat and Matt used was human-first AI: augment the team, don't replace it. That was the part the room responded to, and the part people came up to ask about afterward.
It wasn't just one system
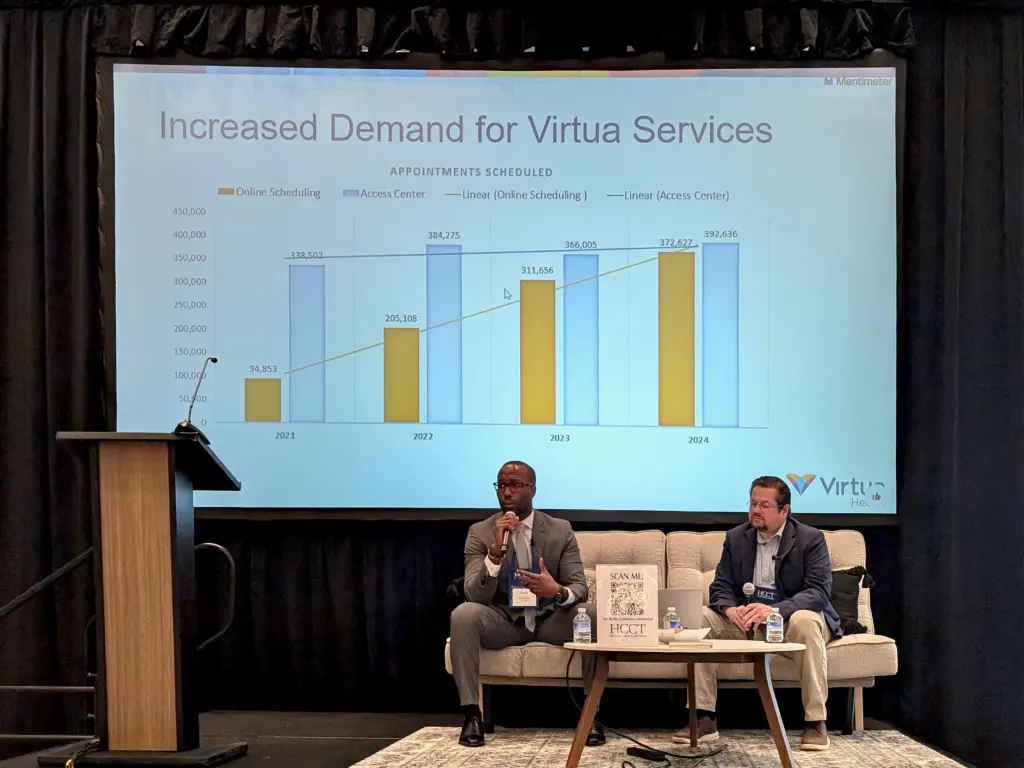
Nebraska Medicine wasn't the only system at the conference showing real results. Virtua runs ActiumHealth agents too, but they have built their program a little differently, and seeing that contrast was the point. Where Nebraska Medicine pointed the agents inward to take volume off their queues, Virtua pointed them outward, using predictive outreach to reach high-risk patients across priority service lines and drive them to the care they needed. Same agents, opposite direction. It showed the range of what these agents can do and the kind of impact they can have across very different organizations.
The takeaway from the floor
That, more than any single number, is what I left HCCT 2026 thinking about. The conversation has moved past whether AI agents work in patient access. Health systems like Nebraska Medicine have already answered that on stage, with their own data. The question now is how fast you can put it to work on the queues that are stretching your team thinnest.
For anyone weighing it: the wait-time math isn't going to get easier, and another hiring cycle isn't going to close the gap. Agentic AI is here now, it is delivering today, and the systems that move on it are the ones handing their staff their day back. If that's the problem on your desk, it's worth a conversation.